


서론
Willis-Ekbom disease (WED)로도 알려진 하지불안증후군(restless leg syndrome, RLS)은 삶의 질, 수면 및 건강에 큰 영향을 미치는 흔한 신경학적 감각운동장애이다[1-3]. 성인의 RLS는 전 세계적으로 약 5-15% 정도로 보고되고 있지만, 인종이나 국가별로 차이가 있다[4]. 국내에서도 유병률이 6.5-8.3%로 외국의 연구와 유사한 수준으로 보고되었다[5]. 젊은 성인에 비해 60세 이상에서 유병률이 2-3배 높은 것으로 지속적으로 보고되며[6], 임상적으로 의미가 있는 RLS는 60세 이상 인구의 3-5%에서 나타나는 것으로 추정된다[7]. 수면의 질과 양을 줄이는 것 외에도 RLS는 야간 보행으로 인한 노인의 낙상 위험 증가와 관련이 있다[8].
RLS의 병태생리에 대한 이해로 뇌의 철분 부족은 널리 알려져 있으며[9,10], 현재 RLS 치료지침들에서는 환자의 철분 상태를 평가하고 철분 저하 시 철분 치료를 시행할 것을 권고하고 있다[11-13]. 따라서 지난 수년간 RLS 및 주기사지운동장애(periodic limb movement disorder)의 경구 및 정맥 내 철분 치료에 대한 과학 및 임상 연구의 수가 증가했다. 최근 이러한 데이터를 평가하기 위해 국제하지불안증후군 연구그룹(International Restless Legs Syndrome Study Group, IRLSSG)은 성인 RLS의 철분 치료에 대한 증거 기반 및 합의지침(evidence-based and consensus guidelines)이 제공되었다[14].
이에 본 종설에서는 국내 상황을 고려하여 RLS의 임상적 진단 및 평가와 더불어 철분 치료를 중심으로 성인 RLS 치료의 지침을 알아보고자 한다.
RLS의 진단 및 평가
1. RLS의 증상 및 진단
RLS는 사지를 움직이려는 강한, 거의 저항할 수 없는 충동을 특징으로 하는 감각운동장애이다. 이러한 움직임의 충동은 사지 안쪽으로 느껴지는 다른 불편한 감각이 항상 동반되는 것은 아니고 종종 간단히 설명하기 어렵거나 불가능한 느낌이 동반되기도 한다. 비록 다리가 가장 두드러지게 영향을 받지만 RLS 환자의 21-57%가 팔의 감각을 표현한다는 점에서 하지불안은 부적절한 명칭이다. RLS를 경험하는 성인들의 대부분은 영어로 이와 같이 표현한다. Restless (가만히 있지 못하는), uncomfortable (불편한), twitchy (움찔거림), need to stretch (스트레칭 필요), urge to move (움직이고 싶은 충동) 및 legs want to move on their own (다리가 저절로 움직일 것 같음)이다. 약 절반은 RLS의 감각을 통증으로 표현한다. Numb (먹먹한) 및 cold (차가운)는 RLS의 감각 증상을 설명하는 매우 드문 표현이다. 최근 발표된 IRLSSG의 진단기준은 Table 1과 같으며[15], 미국수면의학회(American Academy of Sleep Medicine)에서 발행한 제3판 국제수면장애분류(International Classification of Sleep Disorders-3rd edition, ICSD-3)를 최근 대한수면연구학회에서 번역하였다(Appendix 1) [16].
2. RLS의 평가
수면다원검사는 RLS의 평가에 일반적으로 포함되지는 않지만 수면다원검사 연구는 RLS에서 객관적 수면 이상을 보인다. 수면구조에서 지속적인 수면으로 수면잠복기가 증가하며 각성지수(arousal index)가 높다. 하룻밤 수면다원검사를 시행하면 RLS 성인 환자의 70-80%에서 시간당 5회 이상의 수면주기사지운동(periodic limb movements in sleep)이 확인되고, 여러 날 검사를 시행하면 90% 이상의 환자에서 관찰된다. 성인 RLS에서 수면주기사지운동은 수면 전반기 동안 더 두드러지며 밤마다 빈도가 다르다. 수면주기사지운동 각성은 RLS와 동반된 수면 방해에 기여한다. 또한 RLS 감각증상은 다시 잠이 드는 것을 방해하고, 이에 따라 더욱 장기적인 각성을 초래한다[17,18].
RLS의 약물 치료
증상 완화를 위한 대증적 치료로, 항경련제(anticonvulsants, alpha-2-delta [α2δ] ligands), 도파민작용제(dopamine agonists), 레보도파(levodopa), 벤조디아제핀계(benzodiazepine), 철분 제제(iron), 아편양제제(opioid) 등이 사용된다. 도파민 약물은 치료 시작 시 반응이 좋으나 증강현상(augmentation)의 부작용이 점차 알려지며 장기적인 약물 치료에 어려움이 발생하고 있다. 이에 최근에는 α2δ ligands가 1차 약제로 추천되고 있는 추세이며, 이를 고려한 지침이 발표되었다[12]. 1차 약제를 선택할 때 고려해야 할 사항은 Table 2와 같다[12].
RLS의 철분 치료
1. 이론적 근거
여러 연구에 따르면 ferritin이 낮아지면 RLS 중증도가 증가하는 것으로 나타났다[22,23]. 빈혈에서 심한 철분 결핍은 RLS 유병률을 6배 증가시켰다[24]. 빈혈이 없고 말초 철분 저장이 정상인 RLS 환자도 정상 대조군에 비해 뇌 철분은 감소하는 것으로 밝혀졌다[25-27]. 이러한 철 항상성의 뇌 특이적 변화는 RLS에서 볼 수 있는 도파민 이상이 추정 원인으로 간주된다. 따라서 증상만 치료하는 현재 미국식품의약국(Food and Drug Administration, FDA) 승인된 RLS 약물과 달리 철 요법은 근본적인 상대적 뇌 철분 결핍을 교정하여 RLS의 추정 주요 원인을 교정한다[28].
2. 경구 철분제
경구 철분제는 종종 위장장애 및 특정 조건에서 흡수 제한이 있어 순응도가 떨어질 수 있다. 철분 흡수는 적혈구생성(erythropoiesis)과 높은 상관관계가 있기 때문에[29], 적혈구 생산을 위한 충분한 철 저장량이 있는 한 철 흡수에 대한 헵시딘(hepcidin) 의존적 제한이 있을 것이다[30]. 철분 흡수는 혈청 ferritin에 따라 결정되는 철 저장에 영향을 받는데, ferritin이 약 10 μg/L일 때 경구 비헴(non-heme iron) 철의 약 20%가 흡수되지만, 50-75 μg/L 경우에는 1-2% 정도 흡수된다[31]. 따라서 혈청 ferritin이 75-100 μg/L보다 클 때에 경구 철분을 투여하면 이득이 제한될 수 있다.
3. 정맥주사 철분제
정맥주사(intravenous, IV) 철분제는 위장에 의한 조절을 피해 정맥으로 곧바로 투여되어 주로 적혈구계열, 간 및 대식세포에 의해 흡수된다[32]. 대식세포가 뇌를 포함한 다른 기관에 철분을 재분배하는 주요 원천이기 때문에[33], 초기 철분 부하기간 동안 대식세포가 흡수하는 철의 양은 철분이 뇌에 언제, 얼마나 도달하는지를 결정하는 데 관련이 있을 수 있다. 대식세포에 의해 IV 제형에 따른 흡수의 차이뿐 아니라, 운반체 탄수화물(carrier carbohydrate)에서 혈액으로 방출되는 속도의 차이가 있다. 빠른 방출 제제(iron sucrose 및 iron gluconate)는 사용 가능한 transferrin이 압도되어 과도하고 독성이 있는 유리 또는 불안정한 철(free or labile iron)을 생성하는 것을 방지하기 위해 더 낮은 용량으로 투여해야 하며, 원하는 총 용량을 얻기 위해서는 더 낮은 용량을 며칠에 걸쳐 반복해야 한다. 반대로, 느린 방출 제제(low molecular weight iron dextran, ferric carboxymaltose, ferumoxytol, and iron isomaltoside)는 transferrin에 의해 흡수될 수 있는 철분이 더 많이 허락되고 불안정한 철이 덜 발생한다. 느린 방출 제제는 또한 빠른 방출 제제에 비해 대식세포 철 농도의 더 큰 증가를 보여준다[34]. 느린 방출 제제는 1회 또는 2회 반복 투여로 제공될 수 있다. 현재 사용 가능한 IV 철분제 및 기본 특성 목록은 Table 3과 같다[14].
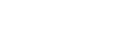
최근 뇌척수액 ferritin 연구는 RLS의 IV 철분 치료에 대한 관심을 되살리는 과학적 근거를 제공했다[25,26]. 뇌척수액 ferritin은 대조군보다 RLS에서 더 낮으며 혈청 ferritin과도 양의 상관관계가 있는 것으로 나타났다[26]. RLS에서 혈청-뇌척수액 ferritin 상관관계는 아래쪽으로 이동하고 약간 낮은 기울기를 갖는 것으로 나타났다(Figure 1) [14]. 이 상관관계는 RLS 환자에서 혈청 ferritin이 200 μg/L 이상으로 증가할 수 있다면 뇌의 철 농도가 정상 대조군에서 볼 수 있는 수준에 도달할 수 있음을 시사한다(Figure 1) [14]. 그러나 이러한 데이터는 개별 변이가 있는 단면 연구이고 뇌척수액 ferritin은 국소 뇌 철분과 제한적인 관계를 가질 가능성이 있다. 그럼에도 불구하고 말초 철분 저장량이 증가하면 잠재적으로 뇌 철분이 증가하고 이후 증상이 감소할 수 있다는 개념을 뒷받침한다. 필요한 것으로 보이는 이러한 더 높은 수준의 말초 철분은 IV 철분으로 달성할 수 있지만 위장관에서 조절되는 흡수를 고려할 때 경구 철분으로는 달성할 수 없다. 이로 인해 RLS에 대한 IV 철분 치료 연구들이 이루어졌으며, 최근 국내에서도 철분정맥투여의 효용성에 대한 연구들이 보고되었다[35-38].
증거 기반 및 합의지침: 성인
1. 경구 철분 치료에 대한 전문가 합의 임상 권장 사항
혈청 ferritin이 75 μg/L 이하인 RLS 환자의 경우, 황산철(II) (ferrous sulfate) 325 mg에 해당하는 경구 철분을 고려해야 한다. 효능이 입증된 연구의 투여 요법은 100 mg 비타민 C (ascorbic acid)를 함께 하루에 두 번 투여했다. Ascorbic acid는 세포 내 환원 메커니즘에 의해 철 흡수를 향상 시키며 철-반응요소결합단백질(iron-responsive element-binding proteins) 및 저산소유도인자(hypoxia inducible factor) 시스템을 조절할 수 있다. 이러한 기전은 전신 및 세포 철 항상성에 중요하다[39]. 새로운 연구는 또한 하루에 한 번 경구 철분을 투여하는 것이 더 빈번한 투여로 더 많은 헵시딘 유도로 인해 하루에 두 번 투여하는 것과 거의 똑같이 효과적이라는 것을 나타낸다[40]. 따라서 임상적 합의에 따라 하루에 1번 또는 2번 투여할 것을 권장한다. 약물을 잘 견디지 못하면 음식과 함께 복용 할 수 있지만 흡수가 감소할 가능성이 있다. 1일 1회 투여는 말초 철분 상태를 증가시키는 이점을 거의 상실하지 않고 부작용을 감소시키기 때문에 1일 2회 투여보다 다소 선호될 수 있다. 격일로 한 번 복용하는 것이 고려될 수 있지만 순응도를 감소시키는 것으로 보인다.
2. IV 철분 치료에 대한 전문가 합의 임상 권장 사항
IV 제제의 투여에 대한 FDA 승인지침을 따라야 한다. Class I 연구에서 IV ferric carboxymaltose 및 유사한 제형이 상당한 증상 개선을 제공하고, RLS에 대한 일차 치료로 사용될 수 있음을 나타낸다[36,41,42]. 그러나 위약 효과를 넘어서는 RLS 증상의 개선은 치료 후 4-6주까지 발생하지 않을 수 있다. 환자 관리는 치료에 대한 이러한 지연된 반응을 계획해야 한다. 이 접근법을 사용한 치료에 대한 적합성을 평가하기 위해 치료 전에 초기 아침 공복 혈액에서 전체 철분 패널을 확보해야 한다. IV 철분 치료 8주 후 아침 공복 혈액에서 반복 철분 패널을 채취하고 8주 후 반복하는 것이 좋다. 권장되는 8주 지연은 IV 철분 치료 후 혈청 ferritin 수치를 상승시키는 급성기 반응 때문이다.
RLS 치료를 위해 경구 및 IV 철분제 사용 시기에 대한 임상적 합의
1. 아래 a와 b가 모두 적용될 때 경구 철분을 사용(치료 알고리즘: Figures 2, 3) [14]
a. 혈청 ferritin은 성인의 경우 ≤75 μg/L, 그리고 b. 다음의 조건은 없음: (1) 경구 철분제에 의해 악화되는 경우(예: 염증성장질환[inflammatory bowel disease]), (2) 경구 철분제가 흡수될 수 없는 경우(예: 비만 수술), (3) 경구 철분제가 빠른 철분 소실을 감당할 수 없는 경우(예: 심한 자궁 출혈, 유전출혈모세혈관확장증 또는 기타 후천혈관형성이상[acquired angiodysplasia]).
2. 경구에서 IV 철분제로 전환
a. 경구 철분제 사용이 어려운 경우, 또는 b. 경구 철분제 사용 12주 후에도 RLS 증상이 임상적으로 의미 있고 혈청 ferritin 또는 기타 철분 측정값이 RLS에 대해 IV 철분제를 제공하는 데 허용되는 값 내에 있는 경우.
3. 경구 철분제가 아닌 IV로 시작
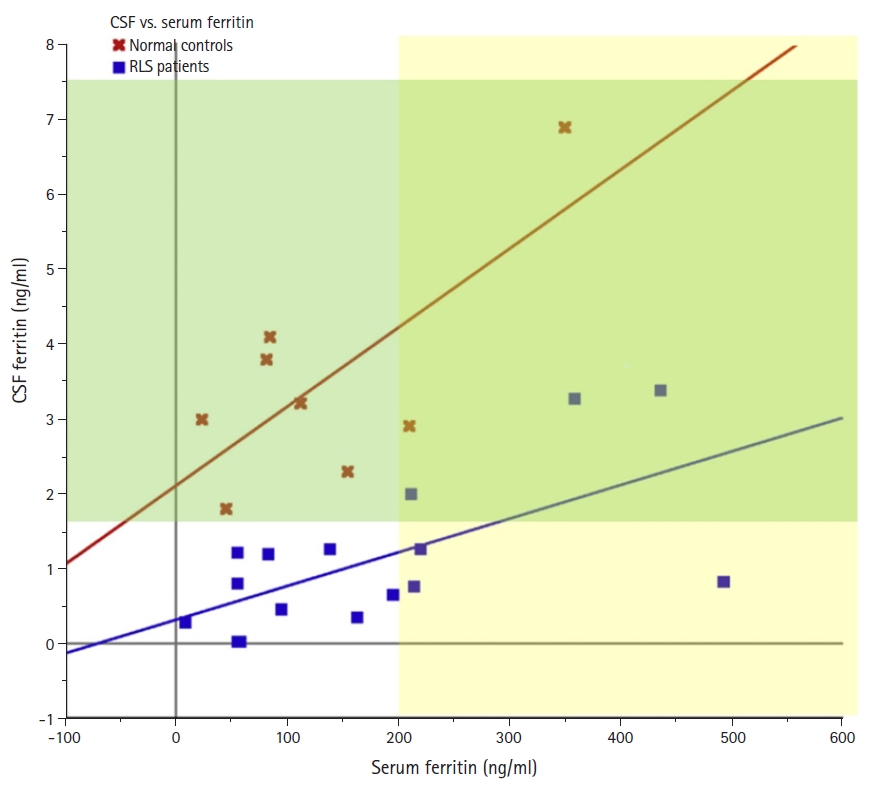
a. 중등도에서 중증(moderate to severe) RLS가 있는 성인: 경구 사용에 대한 의학적 금기 사항이 있지만 IV 철분은 사용하지 않는 경우, b. 다음 중 하나가 있는 경우에만 성인(18세 이상): (1) 혈청 ferritin 75-100 μg/L (또는, 염증으로 혈청 ferritin이 상승하는 경우는 transferrin 포화도가 <20%인 경우에만 IV 철분 치료를 고려), (2) 경구 철분 흡수를 방해할 수 있는 상당한 전신 동반질병이 있는 경우(예: 염증 상태, 류마티스관절염), (3) 과거 경구 철분 치료에 실패한 적이 있는 경우, (4) 경구 철분제로 얻을 수 있는 것보다 더 빠른 증상 완화가 필요한 임상적 상황.
일반적 고려 사항
1. 말초 철분 상태 검사
혈청 철분의 뚜렷한 일주기 변화(아침에 가장 높고 저녁에 가장 낮음), 음식 섭취 직후 혈청 철의 증가, 철분 상태의 독립적 결정 요인으로써 혈청 철분의 중요성 등의 이유로, 철분의 혈청검사는 야간 금식 후 아침에 얻어야 한다. 가능하다면 금식기간 이전의 마지막 식사에는 고기, 특히 붉은 고기의 양이 절제되어야 한다. 전체 철분 패널에는 혈청 ferritin, transferrin 포화도, 철 및 총철결합능이 포함되어야 한다. Soluble transferrin receptor는 매우 비싸고 빈혈이 없는 사람에서는 제한적 가치를 가지고 있기 때문에 일상적인 철분 패널에 포함되어서는 안된다[43]. 실험실 철분검사는 질병 또는 기타 의학적 상태가 있는 하위 집단이 배제되지 않아 철분 지수에 대한 정상 범위에는 빈혈 및 철결핍이 있는 집단이 포함된다. 예를 들어, 혈청 ferritin 15 μg/L는 해당 실험실 결과에서 정상 범위로 나타나더라도 철결핍을 매우 잘 나타낸다[43].
RLS 환자의 초기 평가와 RLS 증상이 이유 없이 악화될 때마다 전체 철분 패널이 권장된다. 반복 철분 패널은 경구 철분 섭취를 시작한 약 3개월 후와 3-6개월마다 변화율을 기준으로 권장된다. 환자가 경구 철분을 사용하는 동안 정기적으로 철분 지수를 확인해야 한다. 환자는 반복 철분 패널을 시행하기 2일 전에 경구 철분을 복용해서는 안된다. IV 철분 주입 8주 후, 이후 8주 후에 다시 철분 상태를 확인해야 한다. 첫 8주 후 철분 평가는 주입으로 얻은 철분 저장 수준을 확인하는 것이다. 두 번째 주입 후 평가는 수준이 얼마나 안정적인지 확인하는 것이다. Transferrin 포화도 >45%이거나 혈청 ferritin >300 μg/L일 때 철 치료를 중단해야 말초 철분 과부하의 위험을 최소화할 수 있다. 혈청 철분 농도는 철분포화도를 계산하는 데 사용되는 두 가지 값 중 하나이므로 이차적으로 철분 값이 상승하면(철제 알약, 금식 실패, 전날 밤 고기를 많이 먹은 경우) 실제 철분포화도를 잘못 추정할 수 있다. IV 철분 치료 후 처음 6주 이내의 혈청 ferritin은 가짜 상승을 보이는 경향이 있으므로 초기 주입 후 8주를 기다리는 것이 좋다. 혈청 ferritin 수치는 염증 과정에 의해서도 상승하기 때문에, 너무 높은 값이라면 다른 철분 측정값과 관련하여 평가해야 한다. 결과에 영향을 미치는 염증이 염려되면 나중에 철분 패널을 반복해야 한다.
2. IV 철분 치료 반응 시간
IV 철분제를 사용한 임상 연구는 전반적인 임상 반응이 지연될 수 있거나 적어도 치료로 얻을 수 있는 최대 효과가 최소 4-6주 지연될 수 있음을 보여주었다. 그러나 일부 환자는 즉각적인 반응을 보고할 수 있다. IV 철분 치료를 시작할 때 환자에게 IV 철분 주입 후 4-6주까지 증상이 호전되지 않을 수 있음을 알리는 것이 중요하다. 추가 치료로 IV 철분제를 사용할 때, 약물 용량을 줄이거나 다른 변경은 증상을 악화시킬 수 있어 IV 철 치료 후 처음 4-6주 동안은 신중히 하거나 하지 말아야 한다.
3. 반복적 철분 치료
IV 철분 치료는 말초 철분 저장을 확실히 증가시킬 것이다. 철분 치료가 철분 상태와 RLS 증상을 개선시킨다면, 결핍의 근본 원인이 재발할 수 있다. 반복적 철분 치료를 결정하는 데 도움이 될 수 있는 임상적 요인은 다음과 같다. (1) 초기 치료에 명백한 증상 이점이 있었는가? (2) 초기 치료에서 혈청 ferritin이 높은 정상 범위로 상승했는가? 아니면 혈청 ferritin이 여전히 정상 범위 중 낮은 수준에서 중간 수준인가? (3) 말초 철분 저장량이 감소하여 증상이 악화되고 있는가? (4) 반복 치료와 관련된 안전문제가 있는가?
성공적인 경구 철분 치료를 반복하기 위한 결정은 혈청 ferritin 수치가 75-100 μg/L 미만으로 떨어짐에 따라 결정될 수 있으며, 이는 RLS 증상을 줄이기 위해 경구 철분을 다시 시작하는 것이 가능한 이점을 나타낼 수 있다. 발표된 Class IV 연구가 하나뿐이고 임상 경험이 매우 제한되어 있기 때문에 IV 철분 치료를 반복할지 여부를 결정하는 것은 더 복잡하기 때문에, 현재로서는 임상지침을 제공할 수 없다. 그러나 위원회의 합의는 이전 초기 IV 철분 치료 연구에서 사용된 ferritin (≥300 μg/L) 및 철분포화도(>45%)에 대한 치료를 제외하는 한계치가 있기 때문에, 반복적 IV 철분 치료를 고려할 때 이를 초과해서는 안된다[36,42].
4. 낮은 말초 철분의 원인 평가
혈액 손실은 철분 상태에서 낮은 혈청 측정치의 가장 가능성 있는 원인이다. 혈청 철분 측정치가 비정상적으로 낮거나 급격히 감소하는 경우에는 혈액 손실의 가능한 원인에 대한 철저한 의학적 평가가 필요하다. 월경과다는 철결핍의 흔한 원인이며, 출혈의 가장 심각한 원인은 위장관 암이다. 흡수장애 또한 철결핍의 일반적 원인이며, 염증장증후군(inflammatory bowel syndrome) 및 복강병, 비만/위 수술 후 흔히 볼 수 있다[43].
결론
RLS는 노인에서 특히 흔한 만성적인 신경계 질환으로, 수면 및 삶의 질에 큰 영향을 미친다. 우리 주변에서 비교적 흔하게 볼 수 있으나, 아직 다른 증상들과 혼돈되어 정확한 진단과 치료지침이 부족한 상황이다.
앞에서 살펴본 이론적 증거 및 임상적 합의를 통해 철분이 RLS에 대한 1차 치료 옵션 중 하나여야 함을 나타낸다. 경구 철분 치료가 주로 첫 번째 선택이 될 것이다. 그러나 경구 철분 흡수를 위한 혈청 ferritin 수치가 너무 높거나, 경구 철분 복용이 어려운 다양한 경우, 구강 철분에 대한 혈청 철분 수치의 반응이 부족한 경우 등에서 IV 철분 투약을 고려해야 한다. 아직 RLS에서 철분 치료의 장기적 이점이나 안전성에 대한 연구는 없기 때문에, 철분으로 치료받은 환자, 특히 IV 철분을 투여 받은 환자는 장기적인 안전을 보장하기 위해 정기적인 추적이 필요하다.
철분 치료는 RLS의 병태생리 및 임상적 증상 개선 등 다양한 측면에서 중요성을 가지고 있다. 향후 보다 적극적인 뇌로의 전달 및 정확한 모니터링 등 치료 방법의 개발이 필요하겠으며, 다양한 임상 연구로 추가적인 장기적 임상지침이 나올 것으로 기대한다.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






