노년기 어지럼
Geriatric dizziness
Article information

Trans Abstract
The prevalence of vertigo and dizziness in the elderly is rapidly increasing due to aging of population. The presence of dizziness in the aged may be connected to falls, which is the leading cause of accidental death in older people. The geriatric dizziness may manifest differently, as patients tend to report less rotatory vertigo and more non-specific and complex dizziness than younger patients. The understanding of pathophysiology in the geriatric dizziness and systematic approach for this symptom help a clinician to find proper management. In this review, we present age-related degenerative changes in nervous system and diagnostic and therapeutic approaches focusing on the elderly patients with dizziness.
서론
어지럼의 유병률은 대규모 집단 연구에서 매년 전체 성인의 15–20%로 보고될 정도로 흔한 증상이며, 남성보다 여성에서 두세 배 더 관찰된다[1]. 나이가 들면서 유병률은 점차 증가하여 영국과 미국에서 조사 결과, 65세 이상 노인의 약 30%에서 어지럼을 경험하며, 85세 이상 노인의 절반이 호소할 정도로 노년기 흔한 증상 중의 하나이다[2]. 이러한 노년기 어지럼은 낙상으로 인한 외상의 중요한 위험요소가 되어, 노인 인구의 약 23%가 일 년에 한 차례 이상 낙상 사고로 연결된다는 유럽에서의 보고도 있다[3]. 이렇게 노년기 어지럼은 2차 사고로 연결될 수 있는 흔한 증상임에도 젊은 성인에게 발생한 어지럼의 양상과 다르게 보고되는 경우들이 많아, 같은 원인이라 하더라도 젊은 성인과 달리 회전성 어지럼은 덜 호소하면서 비특이적인 어지럼으로 혼동을 줄 수가 있다.
이러한 노년기 어지럼의 특성에 대해 분리하여 고찰할 필요가 있기에, 본 종설에서는 노년기 어지럼의 병태생리 및 진단적 접근과 치료에 대해 논의해 보고자 한다.
노년기 어지럼의 병태생리
일반 성인과 같은 원인에 의한 어지럼이라도, 노인의 경우 회전성 어지럼은 덜 호소하면서 막연한 머리 불편감 또는 자세 불안정감 같은 비특이적인 어지럼을 호소하는 경우가 많다[4]. 이는 나이가 들면서 전정기능과 고유감각기능의 저하로 인한 균형감각의 손상과 함께, 여러 경로를 통해 들어오는 감각자극에 대한 중추신경계(central nervous system)의 통합기능 또한 저하됨으로써 모호한 양상의 어지럼을 호소하게 되고[5–7], 젊은 성인에서는 문제를 일으키지 않을 만한 자극에도 어지럼이 쉽게 나타날 수가 있다. 또한, 노년기 근육량과 근력세기의 감소가 더해져 낙상의 위험성이 높아지게 된다[8]. 이러한 노년기 어지럼에 영향을 미칠 수 있는 요소들은 아래와 같다.
1. 전정계의 변화
나이가 들면서 전정기관(vestibular organ)에 위치한 털세포(hair cell) 수와, 상하 전정신경(superior and inferior vestibular nerve)의 신경섬유 수가 감소한다[9–11]. 이로 인한 기능 감소는 반고리관(semicircular canal)에서 가장 크게 나타나고, 그 다음은 소낭(saccule)이며, 타원낭(utricle)의 기능 감소가 가장 적다[12–14]. 이러한 변화로 인해 양성돌발체위현기증(benign paroxysmal positional vertigo)이 발생한 노인은 회전 현기증(rotatory vertigo)은 덜 호소하는 대신, 움직임에 힘들어하고, 자세 불안정감과 불안정한 보행, 특히 갑작스러운 방향전환시 넘어질 것 같다는 호소를 하게 된다[2,15]. 전정기능 감소 시 중추신경계의 보상 역할을 해 줄 수 있는 내측 전정신경핵(mediall vestibular nucleus)의 신경세포 밀도가 감소하고[16], 소뇌의 푸르키네세포(Purkinje cell)의 수도 십 년마다 2.5%씩 감소한다는 보고도 노인의 어지럼 발생에 기여하는 요인이다[2].
2. 말초신경계 및 근골격계의 변화
나이가 들면서 진동감각 및 촉각, 하지 관절움직임의 위치와 방향에 대한 감각과 근력세기도 감소하게 된다[17]. 양측 전정기능저하 발생 시 목의 고유감각기능이 전정기능보상에 중요한 역할을 하는데, 노인에서는 이러한 보상작용이 부족해진다. 시력, 시각 조절(visual accommodation), 깊이 지각(depth perception), 시각 고정 시 안진(nystagmus)이 억제되는 기능의 저하와 함께 신속운동 잠복기(saccade latency)가 늘어나고 안구 추적 속도(eye tracking velocity)도 감소하게 되어, 전정계(vestibular system)의 퇴행변화로 인한 빠른 머리 회전에 대한 보상적 안구운동 능력의 저하가 일어나게 된다[17]. 노인의 근력저하는 자세 변화 시 근력반응의 신속성과 적절성을 감소하게 만든다[8].
3. 중추신경계의 변화
균형유지를 위해서 뇌로 들어오는 신호인 전정감각, 시각, 고유감각을 중추신경계에서 차례로 통합하여 적절한 움직임을 수행할 수 있도록 하여야 하나, 노년기에는 뇌줄기, 소뇌 및 대뇌피질의 신경세포 수의 저하와 수초소실과 같은 퇴행변화로 인해 이러한 통합기능이 떨어지게 된다[12,13,18]. 최근 연구에 의하면 전정기능과 연관된 중추신경계의 통합기능의 장애는 노년기에서 관찰되는 소혈관 백질변성(small vessel white matter disease)과도 관련이 있어 보인다. 소혈관 백질변성이 적은 노인의 경우에는 어지럼의 양상이 좀 더 일반적인 설명가능한 양상을 띠는 반면에, 소혈관 백질변성이 많이 보이는 노인의 경우 모호한 양상의 어지럼을 호소하게 된다[19]. 좀 더 연구가 필요한 부분이지만, 소혈관 백질변성의 양과 침범된 위치에 따라 노년기 어지럼의 양상은 차이가 있을 것으로 보인다.
나이가 들면서 발생하는 균형유지와 관련된 여러 기관들의 퇴행성 변화의 정도가 개개인마다 차이가 남에 따라, 노년기 어지럼의 양상은 정형화된 증상발현보다는 사람마다 다양하게 나타날 수 있음을 염두에 두고 진단에 임해야 한다.
노년기 어지럼의 진단적 접근
노인에서의 어지럼질환은 젊은 성인과 원인 질환은 동일하지만, 2개 이상의 원인이 복합적으로 존재하는 경우도 많이 있다[20,21]. 노년기 어지럼 병력청취 시 반 이상에서 모호하며 일관성 없이 모순되는 증상들을 표현한다[22].
이러한 유형의 환자에게 다음과 같은 체계적인 평가를 통해, 균형과 관련된 각각의 요소와 하부기관에 대한 객관화된 평가가 가능할 것이다. (1) 반고리관의 기능에 대한 평가는 비디오두부충동검사(video head impulse test)를 통해 전정안반사(vestibulo-ocular reflex)를 객관적으로 평가할 수 있다[23]. (2) 소낭과 타원낭의 기능은 전정유발근전위(vestibular evoked myogenic potential)를 통해 평가할 수 있다[24]. (3) 동적체위기록법(dynamic posturography)은 비전정(non-vestibular) 고유감각기능과 시각기능 요소의 중추신경계에서의 통합정도를 평가할 수 있다[25].
그 외, 비디오두부충동검사 대신 병상에서 시행할 수 있는 방법으로, 머리젓기후안진(head shaking nystagmus)과 동적시력검사(dynamic visual acuity)는 쉽고 빠르게 전정안반사를 평가할 수 있는 방법이다[5,6,13]. 기립저혈압, 관절 고유감각 진찰도 비전정 어지럼의 요소를 병상에서 평가할 수 있는 방법이 되겠다[2].
심한 어지럼이 노년기에 갑자기 발생하였을 경우, 뇌졸중의 발생 여부를 배제하는 것은 특히 중요하다. HINTS (head impulse test, nystagmus directionality, and test of skew) 검사의 세 가지 단계 안구운동 평가는 초기 뇌 자기공명영상검사보다도 더 높은 민감도(sensitivity)를 보이므로 이를 활용하도록 한다[26]. 앞서 기술한 대로, 양성돌발체위현기증이 발생한 노인에게서 회전 현기증은 덜 나타날 수 있기 때문에 체위변화 검사(positional testing)도 확인하여야 한다[15].
요약하자면, 노년기 어지럼 환자의 진단적 접근에서 훌륭한 병력청취, 체위변화 검사를 포함한 신경이과적 침상검사(neuro-otologic bedside examination)와 뇌졸중 배제를 위한 평가가 급성기 어지럼 발생시 필수적이라 할 수 있겠다. Figure 1에 노년기 어지럼의 진단적 접근에 대해 모식도로 요약하였다.
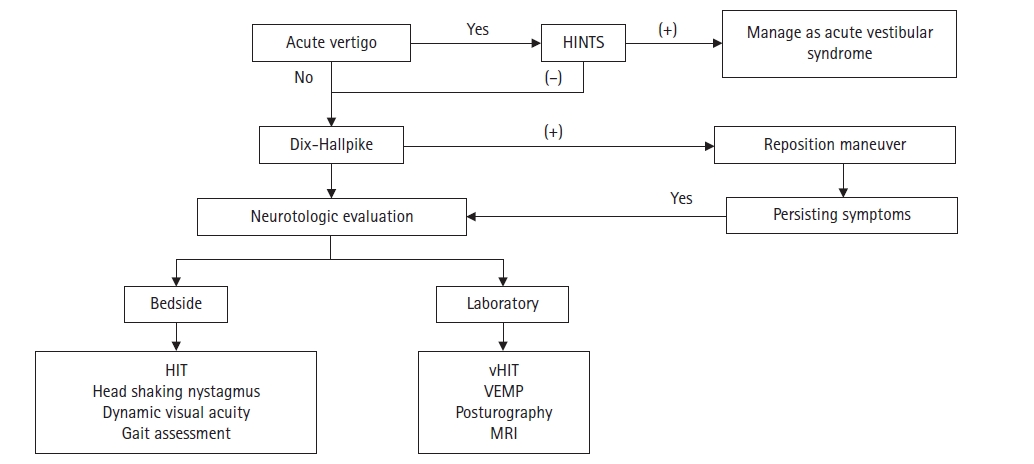
Flowchart for the diagnosis and management of dizziness in the elderly patients. HINT, head impulse test, nystagmus directionality, and test of skew; HIT, head impulse test; vHIT, video head impulse test; VEMP, vestibular evoked myogenic potential; MRI, magnetic resonance imaging.
노년기 어지럼의 원인
노년기 어지럼의 원인은 다른 연령대에서 나타날 수 있는 대부분의 질환이 원인이 될 수 있다. 이는 노출력이 길 수 밖에 없는 점도 작용을 하거니와, 원인 노출 시 노년기에 좀 더 취약하기 때문이다[27]. 노년기 어지럼의 주된 원인을 Table 1에 정리하였다.

Etiology of dizziness and vertigo in the elderly
노년전정장애
2019년 바라니학회(Barany Society)에서 노년전정장애(presbyvestibulopathy)에 대한 진단기준을 발표하였다. 노년전정장애는 경미한 양측 전정장애가 검사소견에서 관찰되면서 자세불안정, 보행 장애 및 넘어짐이 반복되는 노년기 어지럼을 일컫는 질환이라 하겠다. 환자의 병력청취, 침상검사 및 검사실소견으로 진단하게 되며 진단기준은 Table 2와 같다[28].

Diagnostic criteria for presbyvestibulopathy
노년기 어지럼의 질환과 치료
노년기 어지럼도 말초 전정신경계 질환이 가장 흔한 질환이며, 약물치료 및 전정재활(vestibular rehabilitation)로 호전될 수 있다. 급성전정장애의 경우 가능한 한 초기에 전정재활치료를 하는 것이 좋다[29]. 전정재활치료는 적응(전정안반사 네트워크의 재정립), 치환(균형과 관련된 비전정요소의 강화), 습관화(감각역치의 증가)의 원칙에 근거하여 중추보상기능을 촉진시킨다[30]. 약물치료를 시행할 때는 전정 억제제(vestibular suppressant)가 중추신경계의 보상 기전을 억제할 수 있음을 인식하고 짧은 기간 동안에만 사용하는 것이 좋을 것이다[31]. 또한, 이러한 약제 중 노인에게 사용 시 일부 약은 위험을 초래할 수 있어 주의가 필요하다. 예를 들어, 씨나리진(cinnarizine)의 장기간 사용은 우울증 및 파킨슨 증상을 초래할 수 있고, 항히스타민제는 진정작용과 졸림증을 유발하여 낙상의 위험도가 증가할 수 있다[32].
양성돌발체위현기증은 어느 연령대에나 발생할 수 있지만, 나이가 들면서 이석이 분리될 위험도가 높아짐에 따라 50대와 70대 사이에서 가장 호발하게 된다[33]. 원인이 물리적 요소이기 때문에, 약물치료에 대한 반응은 제한적이며 물리적 치료에 기반하게 된다. 이석정복술 시 노년기 환자의 경우 경추부의 움직임에 문제가 있을 수 있음을 감안해야 한다[32]. 양성돌발체위현기증에 대한 약물치료는 노인의 경우 약물상호작용의 가능성이 있으므로 주의하여야겠지만, 다음의 두 가지 경우 약물치료를 고려할 수 있다. (1) 어지럼의 지속(residual dizziness): 이석증 환자의 약 2/3의 환자들이 지속되는 불균형감, 머리 불편감, 피로감 같은 후유증을 6-20일 정도 호소하며, 어떤 환자들의 경우는 한두 달 지속될 수도 있다[34]. 시각과 고유감각계의 기능이 저하되어 있는 노년기 환자는 이러한 어지럼의 후유증이 지속될 수 있어 이 경우, 몇몇 약제(benzodiazepine, dimenhydrinate, betahistine)가 도움이 될 수가 있다[32]. 그러나 앞에서 기술한 것처럼 이러한 약제들은 노년기의 경우 매우 주의하여 짧은 기간 동안 적절한 증상에 사용해야 할 것이다. (2) 양성돌발체위현기증의 재발률은 16–50%로 다양하게 보고되며, 나이가 많을수록 재발률이 높아진다고 알려져 있다[32]. 이러한 재발률과 비타민D 부족이 연관되어 있음이 보고되며[35], 폐경기 여성에서 골다공증의 유병률이 올라가는 것과 양성돌발체위현기증의 재발률과 상관관계가 있음이 보고되기도 하였다[36]. 이러한 결과들에 근거하여, 비타민D의 보충이 양성돌발체위현기증의 재발에 예방적 효과가 있을 가능성이 있다.
중추신경계 질환은 말초 전정신경계 질환보다는 드문 원인이지만 예후와 재활에 미치는 영향을 항시 고려하여야 한다. 최근 백질변성을 포함한 뇌의 소혈관질환과 어지럼이 관계가 있다는 여러 연구들이 보고되고 있다[32]. 노년기 어지럼 환자에게 광범위한 임상적, 전정기관 평가를 하였음에도 뚜렷한 진단이 되지 않는다면 뇌영상을 확인하여 뇌의 소혈관질환 정도를 평가하는 것이 도움이 될 수 있겠다. 소혈관질환이 확인되는 환자들의 경우, 혈압 강하 같은 혈관 위험인자의 조절과 생활습관의 개선이 필요할 것이다.
심인성 어지럼(psychogenic dizziness) 또한 전정 질환과 함께 발생하거나 정신 질환의 증상으로 어지럼이 발생할 수 있다. 이러한 경우 약물치료, 심리치료 및 재활치료가 도움이 될 수 있다. 광범위한 신경이과적 검사에도 불구하고 결론을 내기 힘든 균형이상의 어지럼일 경우, 여러 질환으로 인하여 다양한 복용약을 치료제로 사용하고 있는 상황일 수 있으므로 어지럼의 원인이 여기에 있지 않는지 환자의 투약내역을 확인해야 한다. 몇몇 약제(acetyl-salicylic acid, amiodarone, cisplatin, quinine, furosemide, gentamicin, and streptomycin)는 직접적으로 내이의 달팽이관(cochlear)과 전정기관 수용체(vestibular receptor)에 작용하여 실조증 및 청력저하를 일으킬 수 있다[37]. 또한, 이뇨제(diuretics), 전립선 비대에 사용하는 알파-아드레날린수용체 저해제(alpha-adrenoceptor blocker), 항고혈압제 및 칼슘채널차단제(calcium channel blocker)는 노년기 기립저혈압을 유발할 수 있다[37]. 심장혈관계질환들 중에서는 부정맥, 심부전증, 기립저혈압으로 인한 심박출량의 감소가 노년기 어지럼의 주요 원인이다.
결론
노년기 어지럼의 비특이적 양상은 전정계, 말초신경계, 근골격계 및 중추신경계 전반에 걸쳐 변화가 발생함에 기인하며, 이러한 노년기 특성들을 이해하고 어지럼 환자에게 체계적 접근을 해야 한다. 노년기 어지럼의 원인질환은 다른 연령대와 크게 다르지 않으나, 다른 원인으로 설명되지 않는 노인의 어지럼에서는 최근 발표된 노년전정장애 진단기준에 맞는지 살펴볼 필요가 있다. 노년기 어지럼의 치료는 원인질환에 따라 최소한의 약제를 사용하여야 하며, 광범위한 검사에도 불구하고 뚜렷한 진단이 확인되지 않는 경우 뇌의 소혈관질환에 의한 영향이나 복용약제의 가능성도 고려해야 할 것이다.
Notes
Conflicts of Interest
The author has no potential conflicts of interest to disclose.
Funding
None.